TB-Free India by 2025: We are Befooling Ourselves
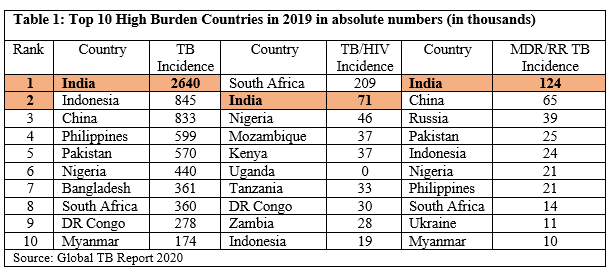
India has maintained its position among the top 20 countries in the recently released global list of high burden countries (HBCs) for tuberculosis (TB), HIV-associated TB and multidrug/rifampicin-resistant TB (MDR/RR-TB) by the World Health Organisation (WHO).
India tops the list in terms of estimated cases per year under two lists – the incidence of TB, and incidence of MDR/RR-TB – in 2019. Under the HIV-associated TB category, India stands at number two after South Africa in terms of estimated TB/HIV cases per year.
On June 17, the WHO released the new lists for 2021–2025, replacing those previously used between 2016 and 2020. The lists provide a focus for global action on TB, HIV-associated TB and drug-resistant TB in countries where progress is most needed to achieve the targets set in WHO’s End TB Strategy. The End TB Strategy is a political declaration of the United Nations (UN) adopted in 2018 for the period up to the SDG deadline of 2030 with specific targets put in place.
India is among the top 10 countries where the burden of TB, HIV-associated TB and MDR/RR-TB is the highest – countries where progress is needed the most to achieve the targets under the End TB Strategy by 2030.
In fact, in terms of India’s achievements in tackling TB, the Global TB Report 2020 makes some alarming observations -
-
India accounts for 26% of the global total of people who developed TB in 2019
-
For Drug-resistant TB, which continues to be a public health threat, India accounts for the highest 27% of the global burden
-
Between 2013-2019 the number of people newly diagnosed with TB increased globally and the biggest contributor was India, where notifications of people newly diagnosed with TB rose from 1.2 million to 2.2 million between 2013 and 2019; an increase of 74%
Unwarranted Policy Complacency within India
On June 24, while chairing the 'TB Mukt Bharat' meeting to review the progress in the fight against TB, Union Health Minister Harsh Vardhan expressed satisfaction over the efforts being made in this regard. He expressed hope that India will be able to eradicate TB by 2025, five years ahead of the global targets. In consonance with this satisfactory stance is the self-congratulatory tone of the India TB Report 2021.
Quite optimistic! However the facts and figures are not encouraging, rather casting doubts over the government's claims of achieving the target of eradicating TB in India by 2025.
While countries such as Cambodia, Chad, and Ghana are no longer in any HBC list, India, despite years of concerted policy pronouncements, continues to remain a high burden country in all the three categories. In fact, it continues to be among the top 10 countries who feature in all the three HBC lists.
“It is very disappointing to see the list. If countries such as Papua New Guinea and Cambodia can transition out of the lists, India could too. Developing policy interventions and making guidelines is important but there needs to be a connect with people’s needs and clear action on the ground. Only having ambitious targets will not help, the government needs to listen to the affected community,” says Blessina Kumar, CEO of the Global Coalition of TB Activists.
A comparison of the current situation with the milestones set towards achievement of targets under the End TB Strategy reveals where India stands –
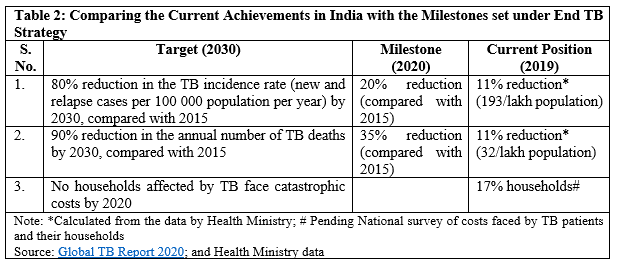
To keep progress towards the targets on track under the Strategy, there are milestones set under each category – milestones in 2020 and in 2025. As per the latest data available, in 2019 – the preceding year of the first milestone – India achieved only an 11% reduction in TB incidence and TB mortality per 1,00,000 population as against the required 20% and 35% respectively. With COVID-19 already proving to be a setback in terms of progress being made under TB, it appears that India is unlikely to achieve the stipulated reductions by 2020.
In terms of catastrophic household expenditure on TB, while the target is that no household faces it by 2020, the latest data for India shows that about 17% of households affected by TB incur catastrophic expenditure. Catastrophic expenditure by a household is defined as expenditure ≥10% of total household consumption or income. The figures for costs incurred, however, are not up to date as India has not yet completed the national survey of costs faced by TB patients and their households.
Impact of COVID-19 pandemic
A number of reports have already pointed out that essential TB services were hit in India due to factors such as reallocation of human, financial and other resources from TB to the COVID-19 response. Studies have also found “considerable disruption in TB service provisions both in the primary care and hospital settings” during the COVID-19 pandemic.
The India TB Report 2021 notes that in 2020, the notifications declined to 1.8 million TB cases, a decline of 25% from the notifications in 2019. This was among the largest drop across countries.
The number of missing TB cases might have increased during the COVID-19 pandemic. There already appear to be some anomalies in the data being provided by the government on missing TB cases. According to the India TB Report 2021, 2.4 million cases were notified during the year 2019, reducing the gap in missing cases to about 0.2 million only. However, the Report of the Joint Monitoring Mission: Revised National TB Control Programme (2019), produced by WHO and Health Ministry, states: “Nearly 0.5 million people with TB disease remain missing to TB surveillance/notification and services.”
Access to Medicines: People Struggling but Government in Denial
One of the major challenges on ground that TB patients and activists face is the availability of medicines, especially for the drug-resistant TB (MDR/RR TB).
In India, the cost of these medicines is exorbitant as these are patented drugs. In November 2020, a representation was filed with the Health Ministry and Commerce & Industry Ministry for considering the grant of a Compulsory License for two drugs– Bedaquiline (BDQ) and Delamanid (DLM) so that lower-cost generic versions of these drugs can be made available.
For persons living with MDR/RR TB, access to oral drugs such as BDQ and DLM is crucial. These new oral drugs for the treatment of DR-TB were developed after a gap of more than 40 years and WHO advocates for replacing injectables, which have severe side-effects, with fully oral therapy for DR-TB using these new medicines.
With no replies from the ministries, a PIL was filed at the High Court of Bombay by two Mumbai-based TB survivors – Meera Yadav and Brinelle D’Souza (petitioner on behalf of the Jan Swasthya Abhiyan, Mumbai) seeking grant of Compulsory License/Government use Authorisation for BDQ and DLM under The Patents Act, 1970.
After orders from the Bombay High Court, the Commerce & Industry Ministry, filed a reply and stated that “all eligible MDR-TB patients were put on an oral regimen treatment (comprising the drugs under reference) free of cost.”
This claim, however, appears to contradict Government’s own document.
According to India TB Report 2021, only 21% of the diagnosed M/XDR-TB cases in 2020 were initiated on newer drug regimen of BDQ and DLM (10,489 out of 50,911 total diagnosed). The figures for total diagnosed already appear to be an underestimate.
Leena Menghaney, a lawyer working on treatment access issues, says that the “ministry is ignoring the ground reality and continuing to hold the position that CL is not required. They have taken the same position in the case of COVID-19 vaccines in the Supreme Court. The people who need the medicines are not being consulted. The government has been repeatedly saying since 2018 that patients will be put on an oral regimen but there is no implementation. Even today reports say that drugs, especially Delamanid, are not available to patients across states. One has to squeeze the drugs out from the system; if you are privileged or get well-connected you get the drugs otherwise not. This is not access!”
Blessina, who has been working as an activist for more than 15 years on the ground, narrates in anguish the case of a 31-year old female DR-TB patient from Uttarakhand who could receive only one month of oral treatment with BDQ. Reverting to injectables has already caused hearing loss, but the oral regimen medicines, which can help avoid such side-effects, are not available in government facilities. Such cases are regularly reported from various states.
While people continue to suffer and struggle for access to these crucial medicines, the government keeps up the hyperbole!
Get the latest reports & analysis with people's perspective on Protests, movements & deep analytical videos, discussions of the current affairs in your Telegram app. Subscribe to NewsClick's Telegram channel & get Real-Time updates on stories, as they get published on our website.