Ebola Epidemic Exposes the Pathology of the Capitalist System
On August 8th the World Health Organisation declared the West African Ebola outbreak a 'public health emergency of international concern'. The declaration came four months after the WHO reported a major Ebola outbreak in Guinea in Western African. Researchers traced the outbreak to a two-year old child who died on 6 December 2013. The epidemic, which broke in Guinea and spread to 3 of its neighbours – Liberia, Sierra Leone and Nigeria – is known to have already affected 2,240 people and killed 1,229. Most public health experts agree that the official figures are a major under-estimation of the extent and spread of the disease.
While large portions of the grossly underdeveloped healthcare systems of Guinea, Liberia and Sierra Leone have virtually collapsed, panic has spread across the world. In Germany, a 30-year-old woman who had returned from Nigeria 8 days back, was rushed to an isolation ward and hundreds who had come in contact with her were quarantined. It later transpired that the woman was, in all probability, not suffering from Ebola infection. Cases have been reported of airlines pilot refusing to fly to the affected countries. The Cameroonian government has decided to close its border with Nigeria. Governments across the world are preparing to put in place measures to quarantine and isolate travellers suspected to be suffering from the infection. Olympic Games organisers have banned young athletes from Ebola-affected regions of West Africa from participating in the Youth Olympic Games in China.
Ebola Epidemics in the past four decades
Ebola infection is not a new disease (or EVD – Ebola Virus Disease as it is now officially termed) and was first reported almost 40 years ago. Formerly known as Ebola Haemorrhagic Fever, simultaneous outbreaks of the disease were reported from Sudan and the Democratic Republic of Congo in 1976. The latter outbreak was in a village situated on the Ebola river – hence the name. It is conceivable that Ebola infections had remained undetected in rural communities much before the identified outbreaks. Since 1976 there have been 24 discrete reports of clusters of infections from different countries in Africa. The following Table provides details of outbreaks where more than a hundred people were reported to have been infected, before the current epidemic.

Five distinct species of the Ebola Virus are known to cause infection, and their virulence (i.e. the ability to cause serious symptoms) varies across these species. While the case fatality rate (i.e. the percent of people infected, who would eventually die) can be as high as 90% for one species, another species which has been known to infect people in China and the Philippines does not lead to fatal outcomes. The Ebola species that is responsible for the present outbreak is not the most virulent, with case fatality rates in the region of 60%.
How Ebola Spreads
Human beings are not the primary targets of the Ebola virus. It affects humans who come in close contact with the blood, secretions, organs or other bodily fluids of infected animals. In Africa, human outbreaks have been traced to the handling of dead or diseased animals such as chimpanzees, gorillas, fruit bats, monkeys, forest antelope and porcupines. The virus is known to have been the cause of major epidemics in chimpanzees and gorillas. All these animals are found in the tropical rainforests, and countries surrounding these have been the centres of Ebola outbreaks. While many animals are known to be infected by the virus, it is now believed that the virus primarily resides in a few species of fruit bats. Unlike other animals infected by the virus, fruit bats do not show any symptoms of disease and thus act as the reservoir for the Ebola virus. What is still a mystery is that the natural habitat of fruit bats lies in Central Africa (where all the earlier major outbreaks had taken place), hundreds of kms. away from the epicenter of the present epidemic in West Africa. It is being hypothesized that there might have been a major shift in the habitat of fruit bats, or that the infection was somehow imported into the region by a human contact.
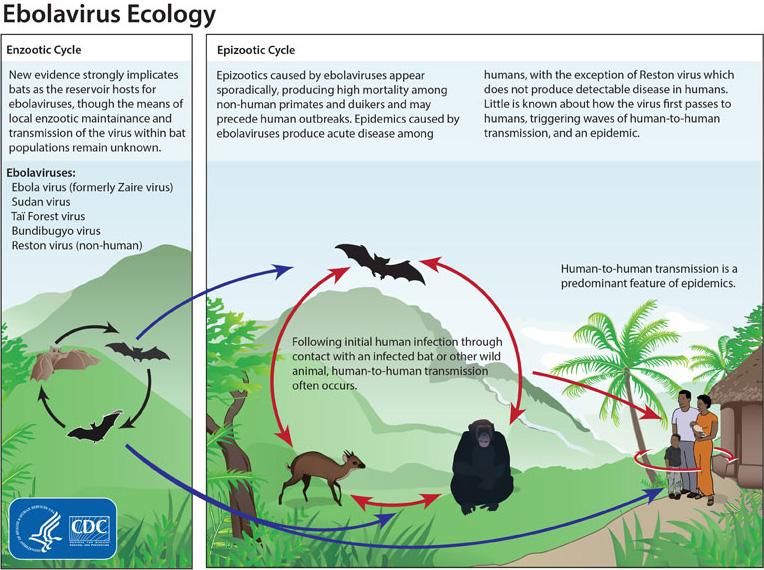
Courtesy: cdc.gov
Once the virus affects a human contact, human to human transmission can take place through direct contact (through broken skin or mucous membranes) with the blood, secretions, organs or other bodily fluids of infected people, and indirect contact with environments contaminated with such fluids. Traditional burial practices, where mourners come in direct contact with the dead, may also be a source of infection. Health workers, who come in contact with infected patients, are particularly at risk when they work in unhygienic conditions (i.e. not adequately protected with gloves, face masks, overalls, etc.). Once infected, a person is capable of infecting others for up to 7 weeks after recovery from illness.
The incubation period of the disease – i.e. the time between when a person gets infected and when s/he shows symptoms, can vary from 2-21 days. The initial symptoms are very like those of other viral infections – high fever, muscle pain, sore throat and headache. Patients often deteriorate rapidly and develop symptoms of vomiting, internal and external bleeding, diarrhoea and rash. The liver and kidneys are most commonly affected. Those who do not succumb to the disease usually make a complete recovery without any residual effects.
There are no approved drugs or vaccines that can treat or prevent the disease. As the disease progresses, the only care possible is supportive – often requiring intervenous hydration and respiratory support.
Not an ideal candidate for an epidemic
There are several typical characteristics that define the disease. The very high case fatality rate sets it apart from most viral diseases that are known to cause epidemics. For example the present Ebola epidemic has a case fatality rate of 60% or more, while even the 1918 influenza epidemic that affected a third of the global population and killed an estimated 50 million people had a case fatality rate of 2.5-5%. Normal influenza epidemics, typically, have a case fatality rate of less that 0.1%, i.e. less than 1 in thousand of those infected would eventually die of the infection. Another feature that sets apart Ebola infection from other infections that cause epidemics is its relatively low level of infectivity. The Ebola virus can enter the human body only when the bodily secretions of an infected person come in contact with broken skin or mucous membrane (i.e. the linings of eyes, mouth, etc.). The third characteristic of importance is that carrier states in humans are not known, and those infected show symptoms of major illness and are relatively easy to identify.
The above three characteristics do not make the Ebola virus an ideal candidate for a major epidemic. As all those who are infected show major symptoms, it would be expected that they would be in a health facility. In which case well know public health safety measure should prevent further spread, as close contact with the infected patient is necessary for the infection to spread.
Why the Epidemic?
Why then are we confronted with an Ebola epidemic in regions of West Africa? The answer lies not in the pathology of the disease but in the pathology of our society and the global political and economic architecture. It is not an accident that the present Ebola epidemic has affected three of the poorest countries in the world. Liberia, Guinea and Sierra Leone number 175, 179 and 183, respectively, out of 187 countries on the United Nation’s Human Development Index. Their health systems are ineffective and almost non-existent in many regions. The present epidemic is an epidemic brought upon by poverty, which in turn is a consequence of the kind of extreme inequity that is fostered by the present capitalist system.
The entire world’s gaze is on these three countries, yet its not just Ebola that is killing people here. Let us take the case of Sierra Leone. Since the beginning of the Ebola outbreak, 848 people have been infected by the virus and 365 people have died. In four months Sierra Leone sees around 650 deaths from meningitis, 670 from tuberculosis, 790 from HIV/AIDS, 845 from diarrhoeal diseases, and more than 3,000 from malaria. These deaths have been occurring for decades, not just in the last four months. Yet global attention was not focused on these countries. For, to do so, would force the rich and the powerful – global leaders, the capitalist press, the institutions of capitalism, the captains of industry, UN agencies – to confront the reality of Africa.
Liberia, Guinea and Sierra Leone are not poor by choice. They did not choose not to build functioning health systems. Centuries of colonial rule left them poor. Imperialist agencies such as the World Bank and the IMF heaped further misery through their infamous structural adjustment programmes. They were instructed not to increase public spending on welfare and public services by these agencies. The WTO promised them the moon in the name of trade liberalisation, and further devastated their economies. The developed capitalist countries send in aid as charity and repatriate back much more through their corporations. These poor countries also subsidise the health systems of rich countries – more doctors born in Liberia and Sierra Leone work in OECD countries than in their home countries. Health worker migration – which is nothing short of a direct subsidy that the poor countries of the world provide to the rich – makes it impossible for West Africa to build credible health systems.
We have known of the Ebola virus for 40 years, yet no vaccine or remedy was ever developed. No pharmaceutical company is interested in a remedy for a disease that afflicts the poor who cannot pay ‘blockbuster’ prices for ‘blockbuster drugs’. Interestingly the only experimental drug that is being discussed (called ZMapp) was developed by a tiny company that runs entirely on public funding. This is also the story of neglected diseases – the story of Kala Azar, Malaria, TB, Chaga’s disease any many more. Diseases that are neglected by the research industry because they do not satiate the hunger of profit hungry pharmaceutical corporations.
Business as Usual?
In the mean time a human tragedy unfolds that is not limited to only those infected by the Ebola virus. The entire health system has been overrun in affected areas, thus amplifying the effect of other diseases. In Liberia's capital Monrovia, at one point all five of the main hospitals were closed. Some have since reopened but are barely functioning. Health workers, scared for their safety, have fled. They are scared with a reason, given reports that gloves, gowns and even safe water is in short supply. One report from Sieera Leone talks about blood, vomit and urine smeared hospital floors. Without protective gear, hospital workers treat Ebola patients wearing only scrubs. When nurses got sick, others went on strike, leaving few people left to pick up patients who had fallen out of their beds.
In some regions the economy is coming to a standstill as people are just too afraid to venture out. Symptomatic of peoples’ distrust of the crumbling health system is the report that residents of the West Point slum in Liberia's capital of Monrovia launched a raid to close down a facility that had quarantined Ebola patients.
So we have an epidemic where there should be none. Routine public health measures are not routine here – they are a luxury that surface during epidemics when provided by global charities. And so the world is worried, lest the infection travels to shatter their comfortable existence. This is the downside of the globalised world that global Capital had not bargained for. If you create conditions where infections fester, they will come back to haunt you. The WHO, which has recently – amidst considerable fanfare – announced a global emergency stands indicted as well. Starved of funding by the US led freeze on financing of UN agencies in the 1990s, it can do little beyond the mouthing of platitudes. Its global budget for outbreak and crisis response efforts is just $109 million—half the level it was even two years ago.
The epidemic, in all probability, will run its course and die down after leaving a trail of death and destruction. Not because we as a global community would have done anything right, but because of the nature of the virus itself. The moot question is, will we have learnt anything? Or will it be back to business as usual?
Disclaimer: The views expressed here are the author's personal views, and do not necessarily represent the views of Newsclick
Get the latest reports & analysis with people's perspective on Protests, movements & deep analytical videos, discussions of the current affairs in your Telegram app. Subscribe to NewsClick's Telegram channel & get Real-Time updates on stories, as they get published on our website.