Kenyan Health Workers Prepare for New Round of Industrial Action

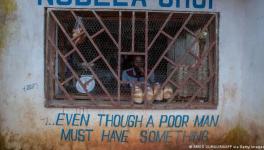
Kenyan medical workers stage a protest. Image credit: Dr. Ayub ( ýobo on dà flag)/X
William Ruto’s government in Kenya has missed another opportunity to address the grievances raised by doctors and other health workers from the Kenya Medical Practitioners, Pharmacists and Dentists Union (KMPDU). Unless there are major changes by the end of Wednesday, March 13, members of the trade union across the health sector plan to walk off their jobs in the early hours of the following day. They are demanding that the government ensure stable employment conditions for health workers, fulfill its obligation to place medical interns in public hospitals across the country, and align incomes with living expenses.
The actions of the workers are unfolding against a backdrop of healthcare reform, which health activists have criticized as an erosion of hard-won rights to meet the requirements imposed by the International Monetary Fund (IMF). This includes replacing the national health insurance scheme with the Social Health Insurance Fund (SHIF), a move the government enforced despite widespread opposition and legal challenges.
Dan Owala, from the People’s Health Movement (PHM) Kenya, told People’s Health Dispatch that although the national insurance model was not perfect —favoring private providers without expanding coverage to the entire population — the SHIF goes a step further by imposing taxes upfront on everyone, regardless of their overall economic status. Even those living in rural areas or working in the informal sector, living on less than USD 1 per day, will be taxed.
To collect the tax, the government is extending its reach beyond salaried workers to include others, using phone records to determine income status based on mobile money transactions, including remittances from family members abroad. The practice is dubious at least.
There is also concern that the latest healthcare reform package, which introduces two additional funds—the Primary Healthcare Fund and the Emergency, Chronic, and Critical Illness Fund—could lead to further opportunities for manipulation and corruption without actually increasing coverage.
“It’s like the World Bank and the IMF themselves have written those laws,” says Owala.
The consequences of the IMF’s loan conditions in Kenya have been chilling, with the country’s debt to the IMF reaching $3.5 billion, including over $940 million USD granted in January 2024 alone. The policies associated with these loans have disproportionately affected poor and working-class communities, with significant increases in the prices of staple foods, fuel, and other materials, leaving 73% of Kenyans in severe financial distress.
This financial strain has also impacted public services, including healthcare, leading to a back-and-forth between the Ministry of Health and the Ministry of Finance. The responsibility for placing medical interns, one of the KMPDU’s main demands, falls on the Ministry of Health, but this can only be accomplished with adequate funding from the treasury, which has not been provided.
The situation is exacerbated by the decentralization of healthcare, with county governments responsible for many health programs but receiving only around 35% of the overall central health budget. They are expected to raise the remaining funds through different donors interested in specific health issues: like tuberculosis or HIV/AIDS.
“The treasury thinks there’s a lot of money coming from donors, but donors don’t fund the health workforce,” Owala points out. In practice, that means money for the health workforce is not coming from any source at all: most donors do not find this heading important enough to fund, while the central government expects hospitals and health centers will find the resources elsewhere.
Donors are also prone to disappear as their interest shifts elsewhere, leaving health services in an extremely precarious position — one that can only be avoided by allocating enough central funding to the overall health system. Contrary to that, health services in Kenya are currently resembling project implementation, where county health providers are expected to submit reports in order to get a new tranche of funding.
The lack of central funding and regressive health reform has had a detrimental effect on health programs, such as Linda Mama. The program was originally introduced in 2016/2017, building upon efforts to strengthen maternity care dating back to the early 2010s. The main aim of Linda Mama was to improve maternal health, including through making maternity services more accessible to those who were left uncovered by the National Health Insurance Fund. The program helped achieve some progress in this field but also, as Owala points out, to somewhat reduce the number of informal abortions.
The SHIF is supposed to take over the purview of Linda Mama and EduAfya, the health benefit package for students, yet doubts remain about how this will be implemented. “We are reversing all the gains we have made,” says Owala.
People’s Health Dispatch is a fortnightly bulletin published by the People’s Health Movement and Peoples Dispatch. For more articles and to subscribe to People’s Health Dispatch, click here.
Get the latest reports & analysis with people's perspective on Protests, movements & deep analytical videos, discussions of the current affairs in your Telegram app. Subscribe to NewsClick's Telegram channel & get Real-Time updates on stories, as they get published on our website.